How many deaths does COVID-19 really cause? As I explained in a previous post, "excess mortality analysis" is a good way to answer this question that avoids problems like missing tests, wrong test results, and incorrect classifications of death. This is an updated look at the excess deaths in the US, and how the number of excess deaths compares to the number of officially reported COVID-19 deaths. I'll start this post with results; details about how the results were calculated are given further below in the post.
Excess deaths in different US states

The graph above shows the excess deaths in the states were affected strongly by COVID-19 early in the pandemic, and later showed decreases in reported COVID-19 deaths, for the weeks ending 3/7 tp 5/16/2020. The numbers shown are the percent of excess deaths, above and relative to the expected deaths for a given week, based on averages from the previous 5 years. For example, New Jersey reported a total of 4,735 deaths for the week ending 4/11, compared to the typical average of 1,441 deaths. The excess of 3,294 deaths is 229% of the expected deaths count. Other states shown in this graph had between about 35% (Colorado) and 150% (New York) additional deaths in the worst weeks.
For comparison, here is a look at "late" states that generally showed a later increase in excess deaths, and no or minimal declines:

There are more states in this list, but the relative increases in deaths are smaller: between 10% and 60%.
The graphs above only extend to 5/16 since too many death report data for recent weeks have not yet been submitted to the CDC. For the weeks shown, most states have reported more than ~90% of the actual deaths, and the CDC spreadsheet tries to estimate the number of missing reports based on historical reporting patterns. However, the CDC estimates are "lowball" estimates that under-predict final numbers, so they cannot be used for the most recent weeks.
Overall, 26 states shown in the graphs above have reported increases in overall mortality between 10% and more than 200% for several weeks in the analyzed time period. Note that the graphs above omit most smaller states because the week-to-week variation in deaths is much larger.
States differ in "COVID-19 death reporting ratios"
In a "theoretically perfect" world, everyone who dies of COVID-19 would be tested for the virus in time, have a positive test result, and therefore have COVID-19 listed on the death certificate; at the same time, nobody who died of other causes would have COVID-19 listed. But tests can fail; people can die alone at home, without ever being tested for COVID-19; doctors and medical examiners can make errors; and other things can go wrong. Looking at the ratio between reported COVID-19 deaths and the number of excess deaths can give a quick impression which of these factors dominate. Here's a graph for all states that reported more than 500 COVID-19 deaths for the 10 weeks 3/14 to 5/16/2020:

Three states have reported more COVID-19 deaths than excess deaths: Connecticut, Washington, and North Carolina. For Connecticut and North Carolina, this is due to very slow reporting of death certificates (see the "Methods" section below). Washington reported 999 COVID-19 deaths and 12,349 total deaths for the 10-week period, which amounts to 882 excess deaths. It is likely that Washington's death reporting is currently at most 99% complete; if so, at least 123 additional deaths will be reported to the CDC over the next months, which will drop the reporting rate to less than 100%.
A closer look at Texas
At the other end of the reporting rate graph is Texas, with 2,973 excess deaths for the 10-week period ending 5/16. The Texas Department of State Health Services data report a total of 1,305 COVID-19 deaths for 5/16, roughly the same as the 1,318 deaths reported by Johns Hopkins. The "Weekly Counts of Deaths by State and Selected Causes" spreadsheet from the CDC shows a total of 1,497 COVID-19 related deaths for this period. This number was reached in the Texas DSHS data on 5/23; this means that COVID-19 deaths totals reported by Texas are one week delayed (which is similar to other states).
However, even considering the delay, only about half of the excess deaths in Texas were attributed to COVID-19.
Of the categories in the CDC "Weekly Counts of Deaths by State and Selected Causes" spreadsheet, only one other category besides COVID-19 shows a large increase over 2019 for weeks 11-20: "Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99)". This includes the R99 classification, which is typically used for death certificates with a "Pending" cause of death that remains to be determined. For Texas, roughly half of these"pending" death certificates appear to get a final classification within two months, and the number of deaths in this category drops to about 1% of total deaths within 4 months.
So the question arises: how many of the "pending" (R99) death certificates will later be classified as COVID-19 deaths?
If most of the pending death certificate would later be classified as "COVID-19", then the reporting rate for Texas would increase substantially, and be in the same range as the New York's reporting rate. But does that happen?
We can see what is happening to the "pending" R99 death numbers over time by looking at the CDC spreadsheets from different weeks. In the graph below, the numbers as shown in the spreadsheet from 5/29/2020 are shown, along with the changes in the most recent spreadsheet that was 4 weeks newer:
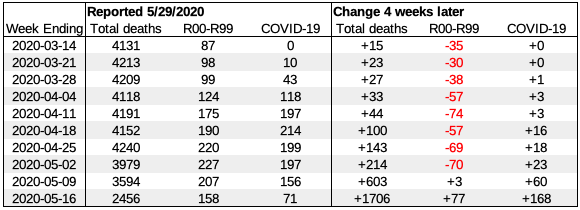
The change in total deaths illustrates that reporting for the last 3 included weeks is only about 60-90% complete. The observed changes show that only a few, if any, of the "pending" death certificates were classified as COVID-19, with a possible exception for the most recent weeks. If we look at the week of 4-11, for example, 74 death certificates were removed from "pending", but the number of COVID-19 cases increased only by 3. Clearly, the vast majority of "pending" deaths were classified in a different category, and not as COVID-19.
Based on this analysis, it appears that Texas reports less than half of the excess deaths linked to COVID-19 are caused by COVID-19. In contrast, COVID-19 is listed as cause of deaths for a larger fraction of excess deaths in most other states. However, in almost all states, the officially reported COVID-19 deaths underestimate the additional deaths significantly - typically by about one third.
For the entire US, the officially reported number of COVID-19 deaths on 5/16/2020 was 89,084; the number of excess deaths during the weeks ending 3/14/2020 to 5/16/2020 was 124,219. Due to incomplete death certificate reporting that is only partly compensated for, the actual number of excess deaths is, in all probability, even higher.
Likely causes of low COVID-19 death reporting rates
There are multiple reasons why the reporting rates for COVID-19 are significantly lower than 100%. They fall into several categories:
- No COVID-19 test results
- False negative test results
- Reporting errors
"many medical examiners and coroners refuse to attribute a death to COVID-19 without a positive test before the person died"
Some medical examiners order COVID-19 tests post mortem, but it is unclear how often this happens. To some extend, such testing can also be subject to political pressure. Even when tests are done, they sometimes can return false-negative results, which makes is less likely that COVID-19 is listed as a cause of death.
For Texas in particular, there are several factors that can cause people to avoid COVID-19 tests. Texas is home to about 1.6 million unauthorized immigrants who may avoid COVID-19 tests out of fear of deportation. Texas also has the highest number of people without health insurance in the nation - 17.7% of the population in 2018, about 5 million people. While federal funds have been made available to test and treat uninsured COVID-19 patients, physician's could register for such funds only after April 27, according to the Texas Medical Association. Many uninsured Texans may have been hesitant to seek tests and treatment, anyway, because they may be responsible for medical costs, for example if no COVID-19 test is ordered. Even political orientation may contribute to avoiding COVID-19 tests: since President Trump has repeatedly stated that "testing makes the US look bad", and that he has "ordered his people to do less testing", some of his avid fans may regard this as a personal instruction to not get tested. If masks have been politicized and are often seen as a sign of "weakness", why would ardent Trump fans think differently of tests? Combine the politicized attitudes towards a public health issue with sudden worsening that is typical for COVID-19, and many of deaths caused by COVID-19 never get reported correctly. Delays in reporting further compound the problem.
Delayed deaths create a false sense of security
At the height of the COVID-19 epidemic in New York, increases in reported COVID-19 cases were quickly followed by increases in deaths:

The delay between the two curves was only about one week.
But the recent increases in cases in the US have shown a different picture - here is a graph for Texas:

Cases have gone up rapidly for about two weeks, but deaths have remained more or less constant. Why?
There are two factors that contribute to the observed differences:
- Longer delays between test results and death reports.
- The current growth of infections is driven by young people.
The primary reason for a longer delay between test results and reports of deaths is increased testing capacities. In New York, testing was so limited that only people with severe COVID-19 symptoms were tested. This means that tests were not done until 10 or more days after the infection. Furthermore, testing was backlogged, and getting results often took several days to two weeks. So on average, test results became available about 17 days after infection. Deaths from COVID-19 happens, on average, about 24 days after infection, and were reported quickly in New York City. This resulted in the observed 7-day offset.
Since then, testing capacities have increased substantially, and backlogs have been eliminated. People can get tested with mild symptoms, and often even before developing any symptoms. On average, test results now are available within about 7 days after infection - 10 days earlier. In addition, the reporting of COVID-19 deaths in Texas appears to be slower by at least several days. Together, this add about two weeks delay, so that we'd expect deaths to rise about 3 weeks after infections started to rise.
The second difference is that the current wave of infections is driven by young people. COVID-19 is much less deadly for younger people, so they were the first to take advantage of states reopening, often pushing the boundaries. As a result, a much higher percentage of young people is now infected, compared to infections that happened in March and April. This also means that for a given number of infected patients, we will see fewer deaths, so the death curve is expected to rise more slowly.
This, however, is only temporary. 20-somethings may be the first to get infected now, but they will pass the infection to their parents, grand parent, coworkers, and others, so that the age distribution will change and more closely resemble the age distribution of the population. As this happens, the death rate will go up - with an additional delay that reflects the "age normalization" of the infection. When COVID-19 deaths shoot up a few weeks from now, it will not really be a surprise - it's perfectly predictable.
Methods
Data files were downloaded from the CDC "Excess Deaths Associated with COVID-19" web page.
Excess death graphs used the "Predicted (weighted)", "All data" data sets. The latest file version downloaded on 6/24/2020 was used unless otherwise noted (data files are updated weekly by the CDC).
For North Carolina and Connecticut, data for the weeks of 5/9 and 5/16 were incomplete or missing, and adjusted to the values of the "Average expected count" column plus the number of COVID-19 cases reported for the week. The total correction was 3,515 additional deaths (2,321 for North Carolina, 1,194 for Connecticut).
To calculate the total excess deaths, the "observed number" values for the 10 weeks ending 3/14/2020 to 5/16/2020 were added, and the total "average expected count" for these weeks was subtracted (after applying the corrections for Connecticut and North Carolina described above). The total number for the US was determined by adding the respective values for all states.
Reported numbers for COVID-19 cases and deaths used are based on Johns Hopkins data files downloaded from Github. COVID-19 death reporting rates were calculated by dividing the number of total COVID-19 death reported on 5/16/2020 by the number of excess deaths for the 10 weeks ending 3/14/2020 to 5/16/2020.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.